Does Wegovy Affect Your Period? What Women Should Know
Wegovy has helped many people lose weight, manage appetite, and improve metabolic health. But for women, one question comes up often: can Wegovy affect your period?
The answer is yes, but usually indirectly. Wegovy is not designed to control the menstrual cycle, and it is not a fertility medication. However, because it can lead to weight loss, appetite changes, insulin changes, and shifts in overall metabolic health, some women may notice changes in their period while taking it.
Some women report delayed or missed periods. Others notice fluctuations in flow, breakthrough spotting, or temporary amenorrhea, which means the absence of menstrual periods. For women with obesity or PCOS, weight loss may also help restore more regular ovulation and menstrual cycles over time.
At Tucson Wellness MD, the goal is to help women understand what is normal, what deserves attention, and when to speak with a provider.
Quick Answer
Does Wegovy affect your period?
Wegovy may affect your period indirectly through weight loss, changes in appetite, reduced calorie intake, improved insulin sensitivity, and hormonal shifts related to body fat changes. Some women may notice delayed or missed periods, lighter or heavier flow, spotting, or temporary amenorrhea. For women with PCOS or obesity-related cycle irregularity, weight loss may help restore more regular cycles. However, any unusual bleeding, pregnancy possibility, severe pain, or prolonged missed periods should be discussed with a doctor.
What Is Wegovy?
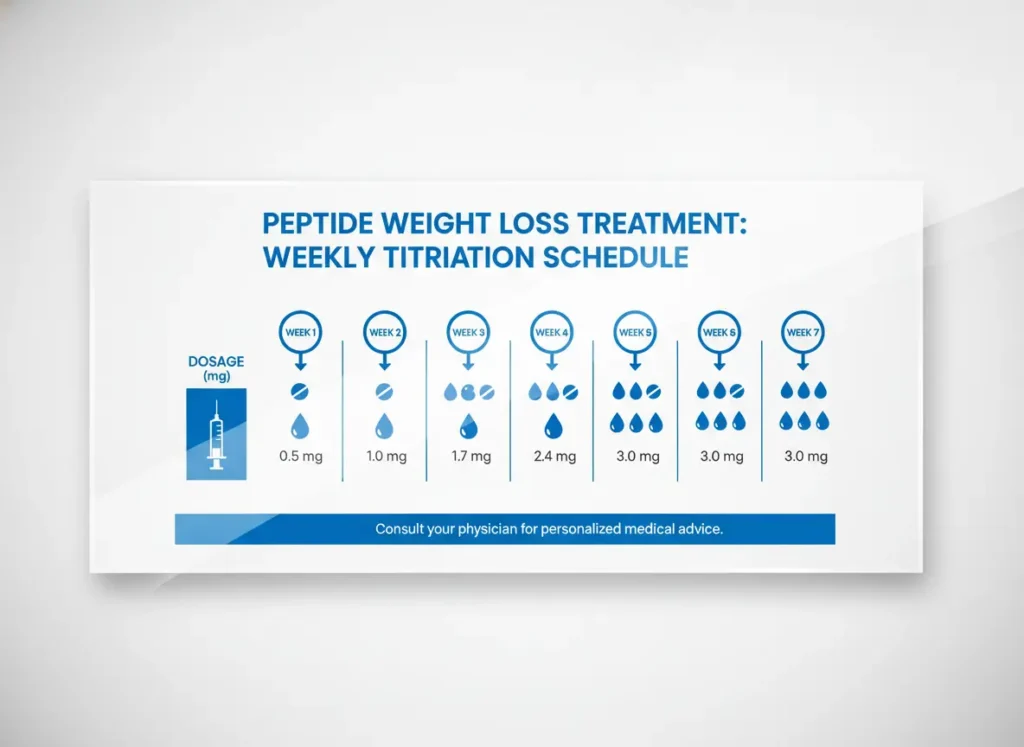
Wegovy is the brand name for semaglutide, a GLP-1 receptor agonist used for chronic weight management in eligible patients. It works by helping regulate appetite, slowing digestion, and improving fullness signals.
Although many people associate semaglutide with peptide therapy because it is peptide-based, Wegovy is an FDA-approved prescription medication. It should only be used under medical supervision.
Wegovy does not directly work like birth control, hormone replacement therapy, or a menstrual medication. Still, the menstrual cycle is sensitive to changes in weight, nutrition, stress, insulin, and energy balance. That is why some women notice cycle changes after starting Wegovy.
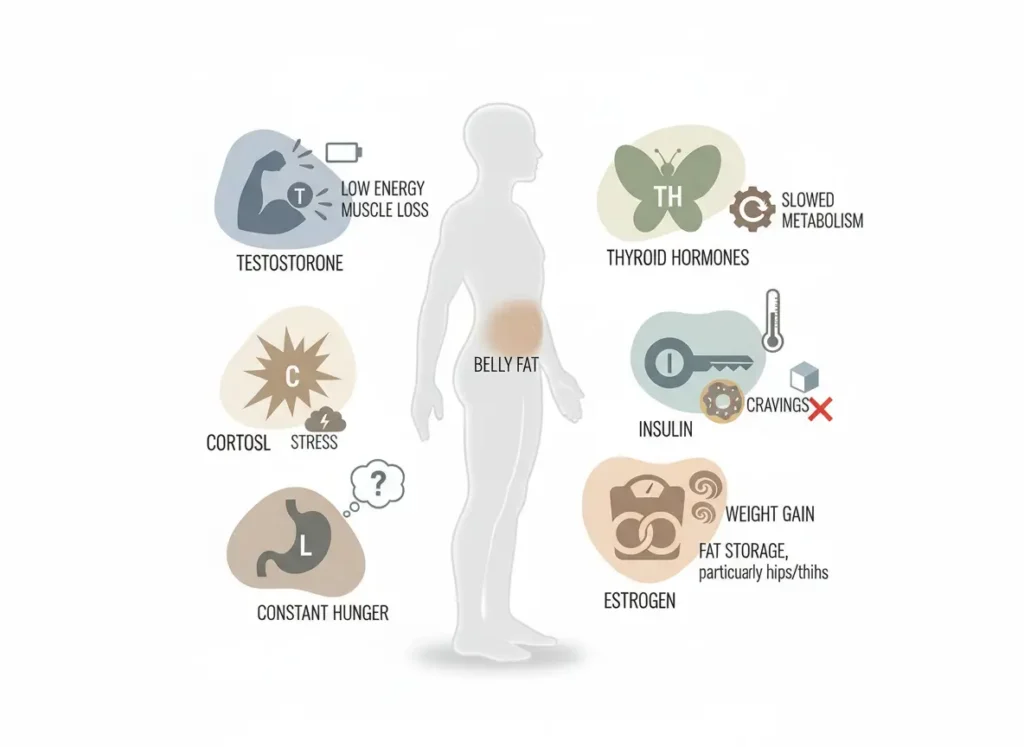
How Wegovy Indirectly Changes Your Period
Wegovy may influence your cycle because weight loss and metabolic changes affect the hormonal system. The menstrual cycle depends on communication between the brain, ovaries, thyroid, adrenal glands, and metabolic signals from the body.
When body weight changes, especially quickly, the body may temporarily adjust reproductive hormone signaling. This can affect ovulation, cycle timing, and bleeding patterns.
Common indirect factors include:
Weight loss
Lower calorie intake
Changes in body fat
Changes in insulin sensitivity
Digestive changes
Stress on the body
Nutrient intake changes
Exercise changes
Improved metabolic health
This does not mean Wegovy is damaging your cycle. Sometimes the body is simply recalibrating. Still, cycle changes should be monitored, especially if they are new, severe, or persistent.
Delayed or Missed Periods
Some women notice that their period comes later than expected after starting Wegovy or increasing the dose. Others may miss a period entirely.
Delayed or missed periods may happen because of:
Rapid weight loss
Eating too few calories
Low carbohydrate or low fat intake
Dehydration
Stress
Exercise changes
Poor sleep
Hormonal shifts
Pregnancy
A missed period should not automatically be blamed on Wegovy. If pregnancy is possible, take a pregnancy test. This matters because fertility may improve in some women as weight loss restores ovulation.
Fluctuations in Flow
Some women may notice that their period becomes lighter, heavier, shorter, or longer than usual. Changes in flow can happen when ovulation timing changes or when the body is adjusting to weight loss.
A lighter period may happen if ovulation is delayed or if overall hormone levels shift temporarily.
A heavier period may happen if your cycle becomes irregular or if the uterine lining builds differently from cycle to cycle.
Occasional changes may not be alarming, but heavy bleeding that soaks pads quickly, bleeding with dizziness, or bleeding that lasts much longer than usual should be evaluated.
Breakthrough Spotting
Breakthrough spotting means light bleeding between periods. This may look like pink, red, or brown spotting.
Spotting can happen for many reasons, including:
Hormonal fluctuation
Birth control changes
Ovulation changes
Stress
Weight change
PCOS
Thyroid issues
Pregnancy
Uterine polyps or fibroids
Infection
Wegovy may be part of the bigger picture, but spotting should not be ignored if it is new, frequent, or accompanied by pain, odor, fever, or pregnancy symptoms.
Temporary Amenorrhea
Temporary amenorrhea means your period stops for a period of time. In the context of weight loss, this can happen when the body senses low energy availability. In plain English, your body may feel like it is not getting enough fuel.
This is more likely if weight loss is very fast or if you are eating too little protein, fat, carbohydrates, or total calories.
Possible signs your body needs more support include:
Extreme fatigue
Hair shedding
Feeling cold often
Dizziness
Poor sleep
Mood changes
Constipation
Skipped periods
Weakness during workouts
If your period stops for several months, speak with a provider. Your care team may need to evaluate nutrition, thyroid function, reproductive hormones, PCOS, pregnancy, stress, or other health factors.
The Positive Impact: Regulating PCOS and Obesity
For some women, Wegovy may have a positive indirect effect on menstrual health. This is especially true for women with obesity, insulin resistance, or PCOS.
PCOS is often linked with irregular periods, insulin resistance, higher androgen levels, acne, unwanted hair growth, and difficulty with weight management. Weight loss can sometimes improve ovulation and cycle regularity.
This does not mean Wegovy is a cure for PCOS. It also does not mean every woman will see cycle improvement. But when weight loss improves insulin sensitivity and metabolic health, reproductive function may improve too.
Restoring Regularity
Some women who had irregular cycles before weight loss may notice more predictable periods after losing weight. This may happen because body fat, insulin, and hormone signaling are closely connected.
More regular cycles may be a sign that ovulation is occurring more often. That can be a good health sign, but it also means pregnancy may become more possible.
This is where the internet’s “Ozempic babies” buzz gets real. Cute phrase, serious reminder. If you do not want to become pregnant, talk with your provider about reliable contraception.
Managing PCOS
For women with PCOS, a comprehensive plan usually works better than relying on one medication. Wegovy may support weight loss, but PCOS care often also includes nutrition, strength training, sleep support, stress management, hormone evaluation, and sometimes medications or supplements.
A PCOS-focused care plan may include:
Weight management support
Insulin resistance evaluation
Nutrition planning
Protein and fiber goals
Strength training
Sleep improvement
Hormone testing
Cycle tracking
Fertility counseling if needed
Natural healing strategies may also support better long-term wellness, but they should be used realistically and safely. PCOS deserves a full plan, not just vibes and green tea.
The Ozempic Babies Phenomenon: Fertility Warnings
“Ozempic babies” is a popular phrase used online to describe unexpected pregnancies reported by some women using GLP-1 medications like semaglutide. The reason may not be the medication directly causing fertility. Instead, weight loss and improved metabolic health may restore ovulation in women who were previously ovulating irregularly.
There is also another practical concern. Vomiting, diarrhea, and delayed digestion may affect how some oral medications are tolerated. If you use oral birth control and experience significant vomiting or diarrhea, ask your provider whether backup contraception is needed.
Wegovy should not be used during pregnancy. Women planning pregnancy are generally advised to stop Wegovy at least 2 months before trying to conceive because semaglutide stays in the body for several weeks.
If you become pregnant while taking Wegovy, contact your healthcare provider right away.
When to See a Doctor
Period changes can happen for many reasons, but some symptoms should be checked.
See a doctor if you experience:
A missed period and possible pregnancy
No period for 3 months or more
Heavy bleeding
Bleeding after sex
Severe pelvic pain
Spotting that keeps returning
Bleeding with fever or unusual discharge
Dizziness or weakness with bleeding
Sudden major cycle changes
Symptoms of thyroid problems
Signs of nutrient deficiency
You should also talk to a provider if you are losing weight very quickly, eating very little, or feeling exhausted. Your weight loss plan may need adjustments to better support hormones, energy, and menstrual health.
How Tucson Wellness MD Supports Women on Wegovy
Tucson Wellness MD helps women approach weight loss with medical oversight and whole-body support. The goal is not only to lose weight, but to protect energy, muscle, hormones, digestion, and long-term wellness.
Depending on your needs, care may include:
Medical weight loss consultation
Wegovy or semaglutide guidance
Peptide therapy discussion when appropriate
PCOS and insulin resistance support
Nutrition and hydration planning
Hormone and metabolic lab review
Cycle tracking guidance
Natural healing strategies
Fertility and pregnancy planning discussions
If your cycle changes after starting Wegovy, do not panic, but do not ignore it either. Tracking your cycle and symptoms can help your provider understand what is happening and whether your plan needs to be adjusted.
Final Thoughts
Wegovy may affect your period indirectly through weight loss, calorie intake changes, improved insulin sensitivity, and hormonal shifts related to body fat and metabolism. Some women may experience delayed or missed periods, fluctuations in flow, breakthrough spotting, or temporary amenorrhea.
For women with PCOS or obesity-related irregular cycles, weight loss may help restore regularity. But improved ovulation also means pregnancy may become more possible, even if your cycles were irregular before.
The safest approach is to use Wegovy with medical supervision, track your cycle, stay nourished, and speak with a provider if changes are unusual, persistent, or concerning.
At Tucson Wellness MD, women receive personalized support for weight loss, hormone health, peptide therapy, and natural healing strategies that fit their goals and health history.
Frequently Asked Questions About Wegovy and Period Changes
Can Wegovy make your period late?
Yes, Wegovy may indirectly contribute to a late period through weight loss, reduced calorie intake, metabolic changes, stress, or hormone shifts. Pregnancy should also be ruled out if there is any possibility.
Can Wegovy cause missed periods?
Some women may miss periods while losing weight on Wegovy, especially if weight loss is rapid or nutrition intake is too low. If you miss multiple periods, speak with a healthcare provider.
Can Wegovy help regulate periods with PCOS?
Wegovy may help some women with PCOS by supporting weight loss and improving metabolic health. This may improve menstrual regularity in some patients, but Wegovy is not a PCOS cure or fertility medication.
Can you get pregnant more easily on Wegovy?
Some women may become more likely to ovulate as they lose weight and improve insulin sensitivity. If you do not want to become pregnant, discuss reliable contraception with your provider.
Should I stop using Wegovy if my period changes?
Do not stop Wegovy without talking to your healthcare provider. Period changes may be temporary, but your provider can help determine whether you need testing, nutrition changes, dose adjustments, or pregnancy guidance.